SOP Reference: MWS-M03-L6
Lesson 6: Dressing Change Frequency Protocols
Clinical indicators for dressing replacement timing and evidence-based wound reassessment criteria in honey therapy management
Clinical Context
Optimal dressing change frequency balances competing priorities: maintaining therapeutic honey concentration at the wound bed, preventing dressing saturation and leakage, minimizing patient pain from repeated dressing removal, and conserving healthcare resources through appropriate use of materials and staff time. Both excessive and insufficient change frequency compromise outcomes.
Dressing changes performed too frequently waste materials, increase patient discomfort, and risk iatrogenic tissue damage from repeated adhesive removal or mechanical disruption of fragile granulation tissue. Changes performed too infrequently allow honey dilution below therapeutic thresholds, permit dressing saturation with overflow onto periwound skin, and delay detection of complications such as infection or deterioration.
Evidence-based protocols establish baseline change intervals based on wound characteristics and treatment phase, then modify frequency in response to clinical indicators observed during dressing removal and wound assessment. This dynamic approach maintains therapeutic efficacy while adapting to the evolving wound environment.
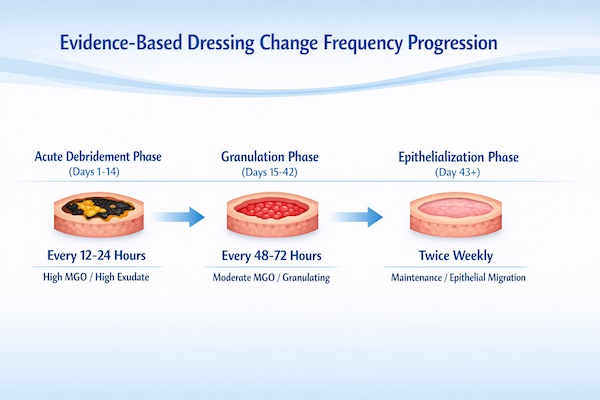
Baseline Change Frequency by Treatment Phase
Acute Debridement Phase (Days 1 to 14)
During active debridement of necrotic tissue or biofilm disruption, wounds require daily dressing changes to maintain high MGO concentration and allow serial assessment of treatment response. Heavy slough production and high bacterial burden generate copious exudate that dilutes honey and saturates dressings within 24 hours.
| Wound Condition | Change Interval | Rationale |
|---|---|---|
| Heavy slough or thick eschar | Every 24 hours | High osmotic draw produces copious exudate; MGO dilution occurs rapidly |
| Suspected or confirmed biofilm | Every 24 hours with mechanical disruption every 48 hours | Prevent biofilm reformation during vulnerable disruption period |
| Purulent infection with systemic antibiotics | Every 12 to 24 hours | Maximize antimicrobial pressure during critical infection control window |
| Post-surgical dehiscence | Every 24 hours for first 7 days | Close monitoring for complications; high exudate in acute phase |
Granulation Phase (Days 15 to 42)
As necrotic tissue clears and healthy granulation tissue fills the wound bed, exudate production decreases and honey concentration requirements moderate. Dressing change frequency can extend to every 48 to 72 hours without compromising therapeutic benefit.
Monitor for signs that longer intervals are appropriate: dressing removal reveals honey still visible on wound bed (not completely absorbed or diluted), secondary dressing shows less than 75% saturation at removal, wound bed appears uniformly granulated without slough reformation, and patient reports decreased pain between dressing changes indicating reduced inflammation.
Epithelialization Phase (Day 43 Until Closure)
During final epithelial migration across the wound surface, honey therapy transitions to maintenance rather than active treatment. MGO concentrations decrease to 100 to 250 milligrams per kilogram, and change frequency extends to every 72 hours or twice weekly.
The goal during this phase shifts from aggressive debridement or antimicrobial control to creating an optimal moisture environment that supports keratinocyte migration. Extended change intervals reduce mechanical disruption that could impair the delicate epithelial sheet advancing from wound margins.
Clinical Indicators for Unscheduled Changes
Mandatory Immediate Change Criteria
Certain clinical findings override the planned change schedule and require immediate dressing removal, wound assessment, and re-dressing. The following situations mandate unscheduled changes:
- Visible Strike-Through: Exudate penetrating through all dressing layers and visible on outer surface indicates complete saturation; continued wear risks periwound maceration and contamination
- Dressing Displacement: Partial or complete dressing detachment exposes wound to environmental contamination and interrupts therapeutic honey contact
- Fecal or Urinary Contamination: Any contact with body waste requires immediate removal to prevent polymicrobial infection introduction
- New-Onset Fever: Temperature above 38.3 degrees Celsius without obvious alternative source suggests wound infection requiring inspection and possible culture
- Severe Pain Increase: Pain escalation exceeding baseline by 3 or more points on numeric scale may indicate dressing-related pressure, infection, or ischemia
- Malodor Development: Strong foul odor permeating through dressing suggests anaerobic infection or tissue necrosis requiring assessment
- Patient-Reported Concerns: Subjective sensation of wound warmth, throbbing, or "something wrong" warrants inspection even without objective findings
Accelerated Schedule Indicators
Some findings do not require immediate change but suggest the current interval is too long and should be shortened. Reassess change frequency if the following patterns appear at two consecutive scheduled changes:
- Secondary dressing consistently saturated at more than 90% capacity
- Honey completely absent from wound bed at removal (indicates dilution to ineffective concentration)
- Periwound skin showing early maceration (white, wrinkled appearance)
- Wound dimensions static or increasing rather than decreasing over 2-week period
- Persistent malodor despite appropriate honey concentration
- Patient reporting pain increase starting 12 to 24 hours before scheduled change
Systematic Wound Assessment at Each Change
Required Measurements and Documentation
Every dressing change, regardless of whether it is scheduled or unscheduled, requires systematic wound assessment and documentation. This serial data collection establishes treatment efficacy, detects complications early, and provides medicolegal protection.
- Wound Dimensions: Measure length and width at widest points using disposable ruler; record depth using sterile cotton-tipped applicator marked at skin level; note any undermining or tunneling with clock-face reference (12 o'clock = head)
- Tissue Types: Estimate percentage of wound bed covered by granulation tissue (red), slough (yellow), eschar (black), or epithelium (pink); goal is progressive increase in granulation and epithelium
- Exudate Characteristics: Document volume (none, minimal, moderate, heavy, copious), color (serous, serosanguinous, sanguinous, purulent), and odor (none, mild, moderate, strong)
- Periwound Skin: Assess for maceration, erythema, induration, warmth, or breakdown; measure any cellulitis extension from wound margin
- Pain Assessment: Record numeric pain scale (0 to 10) both at rest and during dressing change; note any change from baseline
- Photographic Documentation: Obtain standardized wound photograph with metric ruler for scale; maintain consistent lighting and camera distance for serial comparison
Calculating Healing Rate
Wound surface area reduction provides objective evidence of treatment efficacy. Calculate area weekly by multiplying length times width (centimeter squared). Expected healing rate for chronic wounds under optimal therapy is 10 to 15 percent reduction in area per week. Wounds failing to achieve this target despite appropriate honey therapy require reassessment for underlying impediments (ischemia, malnutrition, uncontrolled diabetes, occult osteomyelitis).
Extended Wear Protocols
Criteria for Longer Change Intervals
Select wounds in the granulation or epithelialization phases may tolerate dressing changes every 5 to 7 days, reducing patient burden and healthcare costs. Extended wear requires specific wound characteristics and patient compliance factors:
| Extended Wear Criterion | Required Status |
|---|---|
| Exudate Volume | Minimal to moderate; secondary dressing less than 50% saturated at 72-hour assessment |
| Wound Bed Appearance | 100% healthy granulation tissue; no slough or necrotic tissue |
| Infection Status | No clinical signs of infection for minimum 14 days |
| Healing Trajectory | Consistent 10% or greater reduction in area per week for previous 3 weeks |
| Patient Reliability | Able to monitor for strike-through or displacement and report promptly |
| Dressing Performance | No adherence to wound bed; easy atraumatic removal at 72-hour test change |
Transitioning to Extended Intervals
Move from daily changes to extended wear gradually through intermediate steps. Once daily changes show consistent minimal exudate and complete granulation, trial 48-hour intervals for two changes. If these proceed without complications, advance to 72-hour intervals for two changes. Only after successful 72-hour wear twice should 5 to 7 day intervals be attempted.
Instruct patients to report immediately if they notice dressing saturation, displacement, malodor, increased pain, or fever. Provide clear instructions on how to contact wound care provider 24 hours per day. Any adverse event during extended wear should prompt return to more frequent monitoring until wound stabilizes.
Patient-Centered Considerations
Balancing Clinical Needs with Patient Tolerance
While clinical protocols establish baseline change frequencies, patient-reported pain, anxiety, or lifestyle factors may necessitate modification. A patient experiencing severe pain during dressing removal despite appropriate non-adherent materials may benefit from less frequent changes using longer-acting dressings. Conversely, a patient reporting anxiety about infection may tolerate more frequent changes for peace of mind.
Self-Care and Caregiver Training
For patients managing honey dressings at home, ensure competency in the following skills before discharge from supervised care:
- Aseptic technique including hand hygiene and glove use
- Correct honey volume calculation and application thickness
- Proper dressing removal technique to minimize pain and tissue trauma
- Recognition of infection signs requiring professional evaluation
- Wound measurement and documentation using provided tools
- Appropriate disposal of contaminated dressing materials
- Emergency contact procedures for concerns between scheduled visits
Provide written instructions with photographs demonstrating correct technique. Schedule follow-up visits or telehealth assessments at intervals matching the patient's demonstrated competency level. Weekly professional assessment remains appropriate even for patients performing daily self-care changes.
Cost Considerations and Resource Stewardship
Medical-grade honey and advanced dressings represent significant material costs. Optimize resource utilization by selecting change frequencies that maintain therapeutic benefit without waste. Daily changes during acute debridement justify the material cost through accelerated healing. Extended intervals during maintenance phase conserve resources while supporting continued progress.
For uninsured or underinsured patients, prioritize high-frequency changes during the critical first two weeks of treatment when bioburden control determines success. As the wound improves, transition to longer intervals and potentially lower-cost dressing materials for the maintenance phase.
Monitoring Treatment Response
Expected Progression Milestones
Effective honey therapy produces predictable clinical improvements within defined timeframes. Use the following milestones to assess whether current change frequency and honey concentration support optimal healing:
| Timeline | Expected Finding | Action if Not Achieved |
|---|---|---|
| 48 to 72 hours | Malodor improvement; exudate becoming less purulent | Increase MGO concentration; obtain wound culture |
| 7 days | Visible reduction in slough; granulation tissue appearing at wound base | Consider mechanical debridement; reassess honey application technique |
| 14 days | 50% or more of wound bed showing healthy granulation; exudate decreased to moderate | Evaluate for biofilm; consider biopsy for quantitative culture |
| 21 days | 100% granulation; wound dimensions reduced by 20 to 30% | Imaging for osteomyelitis; vascular assessment; nutritional evaluation |
| 42 days | Epithelial migration visible from margins; wound 40 to 60% smaller | Consider advanced therapies (cellular products, negative pressure, surgical closure) |
Protocol Modification Based on Response
When wounds fail to meet expected progression milestones, systematically evaluate and adjust the treatment protocol. Increase dressing change frequency to daily if currently less frequent. Escalate MGO concentration by one tier (e.g., from 250 to 400 mg/kg to 400 to 600 mg/kg). Add mechanical disruption at every other change if biofilm suspected. Obtain wound culture and consider adjunctive systemic antibiotics if infection suspected despite topical therapy.
Document all protocol modifications with clinical justification. Serial wound photographs provide objective evidence of treatment response or failure independent of dimensional measurements. Wounds showing no improvement after 6 weeks of optimized honey therapy require advanced intervention beyond topical management.
Critical Takeaways
- Baseline change frequency depends on treatment phase: daily during acute debridement, every 48 to 72 hours during granulation, twice weekly during epithelialization
- Mandatory unscheduled changes required for strike-through, displacement, contamination, fever, severe pain, or malodor
- Every dressing change requires systematic wound assessment including dimensions, tissue types, exudate characteristics, and pain score
- Extended wear (5 to 7 days) permitted only for clean granulating wounds with minimal exudate and reliable patient monitoring
- Expected healing rate is 10 to 15% reduction in wound area per week; failure to achieve indicates need for protocol modification
- Wounds showing no improvement after 6 weeks of optimized honey therapy require advanced intervention beyond topical management