SOP Reference: MWS-M03-L5
Lesson 5: Secondary Securing Techniques
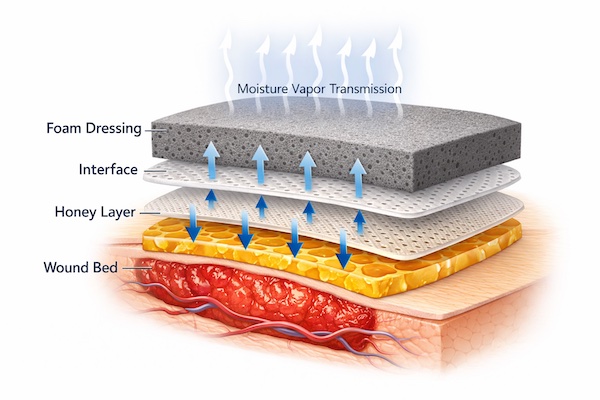
Moisture vapor transmission rate optimization and secondary dressing selection for outer bandage layers in honey-based wound care
Clinical Context
The secondary dressing layer serves three critical functions: absorb excess exudate that passes through the primary honey-impregnated layer, regulate moisture vapor transmission to maintain optimal wound bed humidity, and secure the entire dressing system against displacement from patient movement or environmental stress. Failure in any of these functions compromises treatment efficacy.
Moisture vapor transmission rate (MVTR) represents the key performance metric for secondary dressings. Expressed as grams of water vapor transmitted per square meter per 24 hours, MVTR determines whether the wound environment remains optimally moist, becomes desiccated, or progresses to maceration. Medical-grade honey generates significant osmotic fluid movement that demands precise MVTR calibration to prevent either extreme.
This lesson establishes protocols for secondary dressing selection based on wound characteristics, expected exudate volume, and anatomical location. Understanding MVTR principles allows clinicians to engineer dressing systems that automatically regulate moisture balance without requiring multiple daily assessments.
Moisture Vapor Transmission Rate Fundamentals
MVTR Ranges and Clinical Implications
Different secondary dressing materials exhibit characteristic MVTR values that determine their suitability for specific wound types. The following classification provides guidance for material selection:
| MVTR Range (g/m²/24hr) | Clinical Indication | Representative Materials |
|---|---|---|
| 50 to 500 | Minimal exudate, epithelializing wounds requiring moisture retention | Hydrocolloid outer layers, occlusive films |
| 500 to 1500 | Low to moderate exudate, granulating wounds in maintenance phase | Thin polyurethane foam, composite dressings |
| 1500 to 3000 | Moderate exudate, active debridement or biofilm treatment | Standard foam dressings, absorbent pads |
| 3000 to 5000 | Heavy exudate, venous ulcers, acute wound trauma | Superabsorbent polymers, thick foam with high breathability |
| Above 5000 | Copious exudate requiring multiple daily changes | Absorbent gauze pads, wound pouches with high-capacity reservoirs |
Matching MVTR to Honey Osmotic Load
Medical-grade honey at therapeutic concentrations generates predictable osmotic gradients. Higher MGO concentrations (600 to 1000 mg/kg) produce greater fluid draw and require correspondingly higher MVTR secondary dressings. Lower concentrations (100 to 250 mg/kg) used in maintenance phase tolerate moderate MVTR values without risk of saturation.
As a general principle, when initiating honey therapy at high concentration for debridement or biofilm control, select secondary dressings at the upper end of the MVTR range (3000+ g/m²/24hr). As treatment progresses and honey concentration decreases, step down to lower MVTR materials that extend wear time without compromising moisture balance.
Secondary Dressing Material Categories
Polyurethane Foam Dressings
Foam dressings represent the most versatile secondary layer option for honey-based wound care. The open-cell structure provides high absorption capacity while the polymer backing regulates vapor transmission. Foam thickness directly correlates with absorption volume: thin foams (2 to 3 millimeters) handle low exudate, standard foams (5 to 7 millimeters) manage moderate output, and thick foams (10+ millimeters) accommodate heavy drainage.
- Adhesive Foam: Self-adherent border secures dressing without tape; use when periwound skin tolerates adhesive and dressing changes occur every 3 to 7 days
- Non-Adhesive Foam: Requires separate retention; preferred when periwound skin is fragile or when daily changes necessary during intensive biofilm treatment
- Fenestrated Foam: Pre-cut opening allows wound inspection without complete dressing removal; useful during negative pressure wound therapy integration
- Silicone-Backed Foam: Gentle adhesive for sensitive skin; reduces trauma during removal but costs more than standard adhesive variants
Superabsorbent Polymer Dressings
Superabsorbent polymers lock fluid in gel matrix through chemical binding rather than simple absorption. These materials handle extreme exudate volumes (up to 100 times their dry weight) and prevent lateral fluid migration that causes periwound maceration. Use superabsorbent layers when standard foam saturates within 24 hours despite appropriate sizing.
Superabsorbent dressings are typically non-adhesive and require secondary retention. They work synergistically with honey therapy by removing exudate that would otherwise dilute honey concentration. The gel-lock mechanism prevents fluid return to the wound bed even under compression, making these materials ideal for venous ulcer management under compression bandaging.
Calcium Alginate and Hydrofiber
While typically classified as primary dressings, calcium alginate and hydrofiber materials can serve as secondary absorption layers when honey is applied directly to the wound bed. These materials form conformable gels upon exudate contact, creating a moisture reservoir that prevents wound desiccation between changes.
Layer alginate or hydrofiber over the honey-impregnated primary layer when wound topography is highly irregular or when exudate production fluctuates unpredictably. The gel matrix accommodates volume changes without compromising wound contact. Cover the alginate/hydrofiber layer with an outer foam or absorbent pad to complete the dressing system.
Anatomical Considerations
High-Motion Areas
Wounds over joints or areas subjected to frequent movement (elbow, knee, ankle, shoulder) require secondary dressings with superior mechanical stability. Standard adhesive dressings lift at edges with repeated flexion, creating entry points for environmental contamination and allowing honey to leak onto clothing.
For high-motion anatomical sites, use non-adhesive foam or absorbent pads secured with conformable stretch gauze or cohesive bandages that move with the skin. Avoid circumferential tape application that restricts movement or creates tourniquet effect. Multi-layer tubular bandages provide excellent retention for extremity wounds while accommodating joint flexion.
Dependent Extremities
Leg and foot wounds experience elevated hydrostatic pressure from dependency, increasing exudate production and creating fluid pooling at the most distal wound aspects. Secondary dressings for dependent wounds require higher absorption capacity than anatomically equivalent wounds on the torso or upper extremities.
Select superabsorbent layers or thick foam (10+ millimeters) for dependent wounds, even if exudate volume appears moderate during supine assessment. Encourage leg elevation when possible to reduce hydrostatic pressure. For ambulatory patients, compression therapy reduces capillary leakage and decreases the exudate burden on secondary dressings.
Trunk and Sacral Wounds
Wounds on the back, buttocks, or sacrum face unique challenges from pressure, friction, and moisture exposure from incontinence. Secondary dressings must withstand these mechanical stresses while maintaining absorption capacity.
Use adhesive foam dressings with extended borders (5+ centimeters beyond wound margins) to resist shear forces from patient repositioning. For sacral pressure injuries in incontinent patients, consider transparent film dressings over foam to create a moisture barrier against urine or fecal contamination. Change dressings immediately after contamination events regardless of planned change schedule.
Retention Strategies
Adhesive Border Selection
Adhesive-bordered dressings provide convenient all-in-one retention but require careful application to prevent tension-related complications. The adhesive must be strong enough to resist dressing displacement but gentle enough to avoid epidermal stripping at removal.
| Adhesive Type | Characteristics | Best Application |
|---|---|---|
| Acrylic Adhesive | Strong adhesion, may irritate sensitive skin | Intact periwound skin, high-activity patients, extended wear (5 to 7 days) |
| Silicone Adhesive | Gentle, repositionable, low trauma at removal | Fragile skin, frequent dressing changes, elderly patients |
| Hydrocolloid Border | Moisture-activated adhesion, occlusive properties | Low exudate wounds, moisture retention needs |
| Hybrid Adhesive | Silicone center with acrylic edge for enhanced grip | Moderate activity level, standard wear duration (3 to 5 days) |
Non-Adhesive Retention Systems
When adhesive dressings are contraindicated due to skin fragility, allergy, or frequent change requirements, secure non-adhesive secondary layers with the following materials:
- Conformable Stretch Gauze: Self-adherent gauze wraps secure dressings without adhesive; useful for extremities and areas tolerating light compression
- Tubular Bandages: Elasticized fabric tubes hold dressings in place on limbs; available in multiple sizes for fingers through thighs
- Cohesive Wraps: Self-adhering bandages stick to themselves but not skin; provide compression control and excellent conformability
- Retention Nets: Elastic mesh sleeves for torso, limbs, or head; low-cost option for securing non-adhesive dressings
- Medical Tape: Paper or fabric tape frames dressing edges; avoid circumferential application and remove carefully to prevent skin stripping
Securing Deep Cavity Dressings
Deep wounds filled with honey-saturated packing material require specialized retention to prevent material displacement. Packing that migrates out of the cavity creates voids where biofilm can reform and delays wound closure.
After packing deep wounds or undermined areas, place a primary foam or alginate pad over the packing tail to hold it in position. Secure this pad with adhesive foam or conformable wrap. For wounds with significant depth (more than 3 centimeters), document packing material count at insertion and verify complete removal at each dressing change to prevent retained foreign material.
Special Scenarios
Negative Pressure Wound Therapy Integration
Combining honey therapy with negative pressure wound therapy (NPWT) leverages the antimicrobial benefits of honey while NPWT provides mechanical wound closure forces and continuous exudate removal. Apply honey to wound bed, place non-adherent interface layer, then position NPWT foam and connect to suction.
Set NPWT to continuous suction at 75 to 125 millimeters mercury. The negative pressure draws exudate through the foam into the collection canister, preventing honey dilution. Change NPWT dressing every 48 to 72 hours, reapplying honey at each change. This combination proves particularly effective for deep cavity wounds or those with copious exudate overwhelming conventional dressings.
Compression Therapy Application
For venous leg ulcers, compression therapy addresses the underlying pathophysiology of venous hypertension while honey treats wound bed infection and facilitates healing. Apply honey and primary/secondary dressings first, then apply compression over the dressing system.
Use multi-layer compression bandages (30 to 40 millimeters mercury at ankle) or compression stockings. The compression layers also serve as additional secondary dressing material, absorbing any exudate breakthrough. Change honey dressings per protocol (daily to every 3 days) while leaving compression intact for one week unless saturated. The additional absorption capacity of compression padding often allows less-frequent honey dressing changes as exudate decreases.
Wound Pouching for Extreme Exudate
Wounds producing copious exudate that saturates even superabsorbent dressings within 24 hours may benefit from wound pouching systems. These devices feature an adhesive flange that seals to periwound skin and a drainage port that collects fluid in an external reservoir.
Apply honey to the wound bed, then seal the pouch over the wound. The pouch allows honey to remain in contact with tissue while collecting excess exudate for measurement and disposal. Change pouches every 5 to 7 days when the seal fails; reapply honey at each pouch change. Pouching proves particularly useful for fistulizing wounds or those with combination enterocutaneous drainage.
Troubleshooting Secondary Layer Failures
Premature Saturation
If secondary dressings saturate before the planned change interval, evaluate absorbent capacity relative to wound output. Calculate the saturation time in hours and compare against product specifications. Saturation in less than 24 hours indicates inadequate absorption capacity.
Remedies include increasing secondary dressing thickness (move from 5 millimeter to 10 millimeter foam), adding a superabsorbent layer between primary and secondary dressings, or increasing dressing change frequency to match actual wear capacity. Do not simply extend wear time on saturated dressings, which creates maceration and infection risk.
Dressing Displacement
Secondary dressings that lift, shift, or fall off before scheduled change indicate inadequate retention or inappropriate dressing selection for the anatomical location. Reassess adhesive border width (should extend at least 3 centimeters beyond wound on all sides), evaluate skin preparation (oily or moist skin prevents adhesion), and consider patient activity level.
Switch to stronger adhesive types, add supplemental retention with tape or wraps, or transition to non-adhesive dressings with cohesive bandage retention for high-motion areas. For recurrent displacement, consider body site anatomical factors (excessive hair, skin folds, joint proximity) that may require specialized dressing shapes or retention devices.
Periwound Skin Damage from Adhesive
Repeated adhesive dressing application causes cumulative epidermal injury manifesting as skin stripping, blistering, or allergic contact dermatitis. Prevention requires adhesive selection matched to skin fragility and proper removal technique.
For fragile skin, use silicone adhesive dressings exclusively. Remove all adhesive dressings slowly, pulling parallel to skin surface while supporting the skin with opposing hand pressure. Never pull perpendicular to skin, which creates shear forces that strip epidermis. If skin damage occurs, switch to non-adhesive dressings with tape-free retention for two weeks to allow healing.
Critical Takeaways
- Moisture vapor transmission rate (MVTR) is the key metric for secondary dressing selection, ranging from 50 to over 5000 g/m²/24hr
- Match MVTR to honey osmotic load: high MGO (600 to 1000 mg/kg) requires high MVTR (3000+); low MGO (100 to 250 mg/kg) tolerates moderate MVTR
- Polyurethane foam dressings offer versatility for most wound types; superabsorbent polymers handle extreme exudate
- High-motion areas require non-adhesive dressings with cohesive wrap retention to prevent displacement
- Compression therapy for venous ulcers serves dual purpose: addresses pathophysiology and provides additional absorption capacity
- Premature saturation indicates need for higher-capacity materials or more frequent changes, not extended wear on saturated dressings