SOP Reference: MWS-M03-L4
Lesson 4: Primary Layering Techniques
Direct contact application strategies for honey-impregnated dressings ensuring optimal wound bed interface and sustained therapeutic delivery
Clinical Context
The primary dressing layer establishes direct contact with the wound bed and serves as the delivery vehicle for medical-grade honey. This interface layer must accomplish competing objectives: maintain intimate contact with irregular wound surfaces, prevent adherence that causes trauma during removal, allow bidirectional fluid movement (honey into wound, exudate into secondary dressing), and preserve honey's antimicrobial concentration throughout the wear period.
Poor primary layer selection or application technique undermines the entire treatment protocol. Dressings that adhere to granulation tissue cause pain and bleeding during removal, re-traumatizing the wound and delaying healing. Dressings with inadequate honey retention allow rapid dilution by wound exudate, reducing MGO concentration below therapeutic thresholds within hours. Dressings that fail to conform to wound contours create dead spaces where honey cannot reach, leaving untreated areas vulnerable to biofilm development.
This lesson establishes evidence-based protocols for primary layer selection and application that optimize therapeutic delivery while minimizing patient discomfort and iatrogenic tissue damage.
Primary Dressing Categories
Commercial Honey-Impregnated Products
Pre-manufactured honey dressings deliver standardized MGO concentrations in ready-to-use formats. These products eliminate concentration variability but cost significantly more than bulk honey with separate dressing components. The following categories represent the primary commercial options:
| Product Type | Construction | Best Application |
|---|---|---|
| Calcium Alginate Sheets | Alginate fibers saturated with medical-grade honey (80% honey by weight) | Moderate to heavy exudate wounds; alginate absorbs fluid while maintaining honey contact |
| Hydrocolloid-Honey Matrix | Hydrocolloid base with dispersed honey particles in gel suspension | Minimal exudate wounds requiring extended wear time (48 to 72 hours) |
| Tulle Gauze | Open-weave gauze impregnated with honey (approximately 70% coverage) | Shallow wounds, skin grafts, donor sites requiring non-adherent contact |
| Polyurethane Foam | Open-cell foam saturated with honey throughout matrix | Deep cavity wounds, undermined areas needing void-filling capacity |
| Hydrogel Sheets | Cross-linked polymer gel with honey suspension (60% water content) | Dry eschar requiring moisture donation before debridement |
Bulk Honey with Separate Interface Dressings
For facilities managing high wound volumes, applying bulk medical-grade honey with separate non-adherent contact layers offers cost advantages. This approach requires additional training to ensure consistent honey application thickness and appropriate dressing selection, but provides flexibility in MGO concentration adjustment and dressing architecture customization.
Direct Honey Application Protocol
Wound Bed Preparation
Before honey application, the wound must be clean, debrided of non-viable tissue, and irrigated to remove surface exudate and debris. Pat the wound bed dry with sterile gauze, removing excess moisture that would dilute honey concentration immediately upon application. Moisture in the wound base is acceptable, but pooled fluid requires removal.
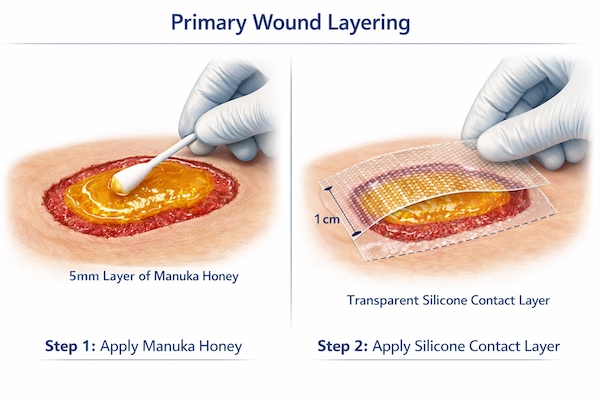
Application Technique for Shallow Wounds
For wounds less than 5 millimeters deep with intact margins, apply honey directly to the wound surface using a sterile applicator or tongue depressor. Spread evenly to achieve uniform thickness of 3 to 5 millimeters across the entire wound bed. Extend honey coverage to within 2 millimeters of wound margins but avoid contaminating intact periwound skin, which risks maceration.
- Dispense the calculated honey volume onto a sterile field (estimate 1 milliliter per 5 square centimeters of wound surface)
- Using sterile applicator, transfer honey to wound bed in systematic pattern (e.g., center outward in spiral)
- Ensure complete coverage of all wound base irregularities including undermined edges
- Verify uniform thickness by visual inspection; areas of thin coverage appear translucent
- Apply non-adherent contact layer immediately before honey spreads beyond wound margins
Application Technique for Deep Cavity Wounds
Wounds deeper than 1 centimeter or with significant undermining require modified technique to ensure honey reaches the wound base. Simple surface application leaves the cavity untreated, creating anaerobic pockets that foster infection.
For deep wounds, loosely pack the cavity with honey-saturated alginate rope or ribbon gauze, working from the deepest point toward the surface. Avoid tight packing that increases pressure and impairs circulation. The goal is to fill the void space with honey-laden material that maintains contact with all cavity surfaces. Leave rope end visible at wound surface to facilitate atraumatic removal at dressing change.
Non-Adherent Interface Selection
Material Compatibility with Honey
The interface layer placed over bulk honey must prevent dressing adherence while allowing honey and exudate transmission. Material selection significantly impacts clinical outcomes, as some dressings absorb honey from the wound bed while others create impermeable barriers that trap exudate.
| Interface Material | Honey Compatibility | Clinical Notes |
|---|---|---|
| Silicone Contact Layer | Excellent - minimal honey absorption, easy removal | Preferred for fragile granulation tissue; expensive but reduces dressing change pain |
| Petroleum-Impregnated Gauze | Good - petrolatum repels exudate but allows honey contact | Cost-effective for daily changes; petrolatum may reduce honey adhesion to wound |
| Perforated Plastic Film | Fair - prevents adherence but may trap exudate if holes too small | Ensure large perforation size (3+ mm diameter) for adequate drainage |
| Plain Gauze (Dry) | Poor - adheres to wound bed, absorbs honey rapidly | Not recommended; causes pain at removal and wastes honey through absorption |
| Hydrocolloid Sheets | Incompatible - impermeable barrier prevents exudate transmission | Do not use as primary interface over honey; traps fluid and increases infection risk |
Sizing and Overlap Principles
Cut the non-adherent interface layer to extend approximately 1 centimeter beyond wound margins in all directions. This overlap prevents honey migration onto intact skin while ensuring the interface protects all granulation tissue from secondary dressing contact. For irregularly shaped wounds, template the wound outline on sterile paper first, then cut the interface layer using the template as a guide.
Special Considerations for Wound Topography
Undermined Wounds
Undermining creates tunnels extending beneath intact skin margins where conventional honey application cannot reach. These spaces harbor bacteria in protected environments and impede healing. Management requires specialized packing techniques.
Use alginate rope saturated with honey to pack undermined channels. Insert the rope gently using sterile forceps or a cotton-tipped applicator, working from the deepest extent toward the wound opening. Fill the undermined space loosely without applying pressure that could extend tissue separation. Leave rope tail visible at tunnel entrance for easy removal. Change packing daily during active undermining; as the tunnel fills with granulation tissue, decrease frequency to every 48 hours.
Sinus Tracts
Sinus tracts represent narrow epithelialized channels connecting the wound surface to deeper structures such as bone, foreign bodies, or abscesses. Unlike undermining, sinus tracts have defined walls and often indicate osteomyelitis or retained foreign material.
Honey packing provides antimicrobial benefit but cannot resolve the underlying pathology. Pack loosely with honey-saturated gauze or alginate to maintain tract patency and suppress bacterial growth while pursuing definitive treatment (surgical exploration, bone debridement, foreign body removal). Monitor tract depth weekly; failure to shorten over 3 weeks despite honey therapy indicates need for surgical intervention.
Irregular Wound Surfaces
Wounds with irregular contours (pressure injuries over bony prominences, surgical dehiscence along curved incision lines) create challenges for uniform honey distribution. Honey applied to elevated areas migrates to dependent zones under gravity, leaving portions of the wound uncovered.
For irregular topography, use honey-impregnated foam or alginate sheets that conform to wound contours and maintain positional stability. Alternatively, apply honey in slightly thicker layers (up to 7 millimeters) at elevated wound areas, accepting that some honey will redistribute during wear but ensuring all areas receive therapeutic coverage.
Primary Layer Troubleshooting
Adherence Despite Non-Stick Interface
If the primary dressing adheres to granulation tissue despite use of appropriate non-adherent materials, evaluate the following potential causes:
- Interface Layer Too Small: Ensure 1 centimeter overlap beyond all wound margins; inadequate overlap allows secondary dressing to contact wound edges directly
- Excessive Wear Time: Dressings left beyond recommended change interval may incorporate into granulation tissue as epithelial cells migrate; reduce wear time
- Inadequate Honey Volume: Insufficient honey allows interface layer to contact wound bed directly; increase honey thickness
- High-Friction Dressing Removal: Pulling dressings perpendicular to skin creates shear forces; instead, support wound edges with one hand while gently lifting dressing parallel to skin surface
Honey Dilution and Loss of Efficacy
In highly exudating wounds, wound fluid dilutes honey concentration below therapeutic thresholds within 12 to 24 hours. Signs of dilution include thin, watery appearance of honey at dressing removal and lack of expected antimicrobial response (persistent odor, stalled healing).
Combat dilution through increased honey concentration (move from 250 mg/kg to 400+ mg/kg MGO), thicker application layers (5 to 7 millimeters instead of 3 millimeters), more frequent dressing changes (daily instead of every 48 hours), and improved exudate management using higher-capacity secondary dressings that reduce hydrostatic pressure driving fluid back into the wound.
Periwound Maceration from Honey Migration
Honey extending beyond wound margins onto intact skin causes maceration characterized by white, wrinkled, fragile epidermis. Prevention requires meticulous application technique and protective barriers.
Apply liquid skin protectant (cyanoacrylate or acrylate polymer) to periwound skin before honey application. Alternatively, frame the wound with strips of hydrocolloid or foam dressing, creating a raised border that contains honey within the wound bed. If maceration develops, temporarily reduce honey thickness and apply zinc oxide paste to affected skin until integrity restores.
Documentation and Quality Assurance
Primary Layer Documentation Requirements
Each dressing change should document the following elements to ensure protocol consistency and support quality improvement:
- Type of primary dressing used (commercial product name or bulk honey plus interface type)
- Honey concentration (MGO mg/kg)
- Estimated honey volume applied (milliliters)
- Application layer thickness (millimeters)
- Interface material and size
- Wound bed appearance before and after application
- Patient pain score during application and at rest
- Ease of dressing removal at subsequent change (adherence, bleeding, pain)
Training Verification for Honey Application
Clinical staff applying medical-grade honey should complete competency verification demonstrating proper technique. Competency assessment includes correct honey volume calculation, aseptic application without periwound contamination, appropriate interface layer selection and sizing, and atraumatic dressing removal technique. Annual re-verification maintains skill consistency across the wound care team.
Critical Takeaways
- Primary dressing establishes direct wound bed contact and determines therapeutic delivery efficacy
- Apply honey in 3 to 5 millimeter uniform layer covering entire wound base; avoid contaminating intact periwound skin
- Silicone contact layers provide optimal non-adherence for fragile granulation tissue; petroleum gauze offers cost-effective alternative
- Deep wounds and undermining require honey-saturated packing materials (alginate rope, ribbon gauze) to reach all surfaces
- Interface layers must extend 1 centimeter beyond wound margins to prevent secondary dressing adherence
- Combat honey dilution in high-exudate wounds through increased concentration, thicker layers, and more frequent changes